

Your arm goes limp after a collision. The shoulder burns like electricity, and your hand won’t respond the way it should. These aren’t muscle problems; they can signal a brachial plexus injury, a form of nerve damage that’s frequently underestimated and sometimes missed entirely in initial trauma evaluations.
The brachial plexus is a network of nerves running from the lower cervical spine through the shoulder and into the arm and hand. When this network is disrupted, outcomes vary dramatically: temporary weakness in mild cases, permanent paralysis in severe ones. What determines where a patient lands on that spectrum isn’t visible on a standard X-ray; it requires a focused neurological assessment. Brachial plexus nerve damage affects every layer of arm function simultaneously: movement, sensation, and strength.
What the Brachial Plexus Is and Why It Matters
The brachial plexus is built from five nerve roots (C5 through T1) that exit the spinal cord between the cervical vertebrae. These roots converge and reorganize into trunks, divisions, cords, and then terminal branches: the median, radial, ulnar, musculocutaneous, and axillary nerves. Together, they govern virtually every movement in the shoulder, elbow, wrist, and hand, as well as sensation across the entire upper extremity.
What makes this system anatomically exposed is its course. It passes through a narrow corridor between the collarbone and the first rib, continues under the pectoralis minor, and runs into the armpit. Any force that widens the angle between the head and the shoulder, or suddenly drives the shoulder downward, places those nerve roots under acute mechanical tension.
A brachial plexus injury doesn’t isolate itself neatly. The entire integrated network is affected, which explains why two patients with apparently similar accidents can present with entirely different deficits.
How Brachial Plexus Injuries Happen
Brachial plexus injuries follow predictable patterns based on the mechanism of force. High-speed motorcycle and car accidents are the leading cause – the shoulder is driven downward while the head snaps to the opposite side, placing the upper nerve roots under sudden, extreme tension. Contact sports reproduce this in a lower-energy form: football players tackled into the ground, with the neck forced sideways, experience what athletes call a “stinger” or “burner.”
Birth trauma is a significant cause in pediatric patients. When excessive lateral force is applied to a newborn’s head during a difficult delivery, the upper roots (C5–C6) are most vulnerable – a pattern that produces what’s known as Erb’s palsy.
Falls from height, gunshot wounds, and stab wounds round out the picture. What matters clinically is not just the event but the nature of the force – stretch, compression, or laceration – because each produces a distinct injury pattern with its own prognosis.
Types and Severity of Nerve Damage
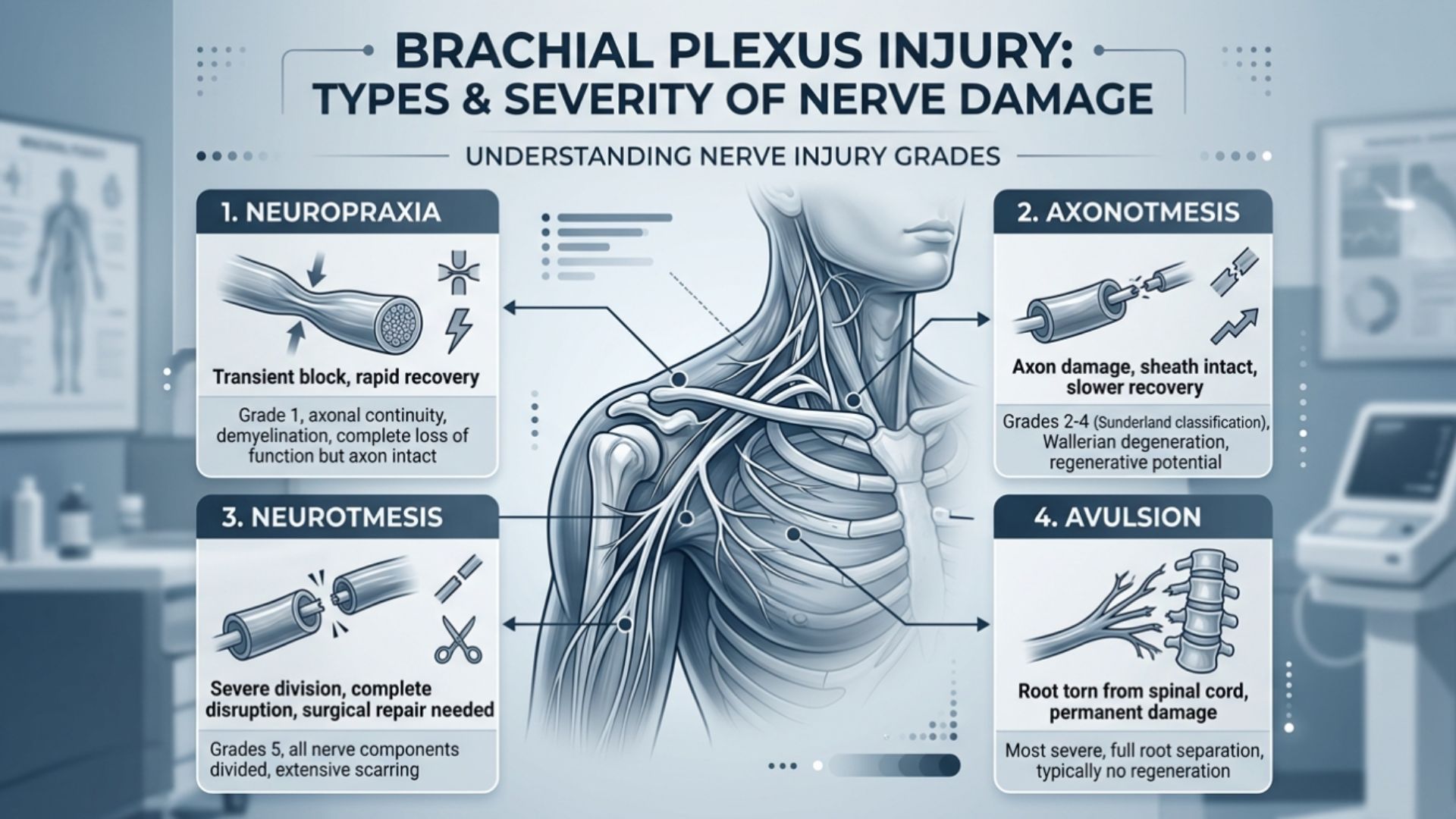
Not all nerve injuries are equal. Neurologists use a four-level classification that directly shapes treatment decisions and recovery expectations:
- Neuropraxia is the mildest: the nerve is stretched but not torn, and the myelin sheath is temporarily disrupted. Function typically returns within weeks, no surgery required.
- Axonotmesis involves damage to the axons themselves, while the outer nerve sheath remains intact. Regeneration is possible but slow – roughly one inch per month – meaning recovery unfolds over many months even in favorable cases.
- Neurotmesis is a complete nerve tear. The nerve cannot regenerate on its own; surgical intervention is necessary to restore any meaningful function.
- Avulsion is the most severe: the nerve root is pulled entirely from the spinal cord and cannot be reattached directly.
Brachial plexopathy is the clinical term for dysfunction across this nerve network – the underlying pathological process. Brachial plexus palsy describes what the patient actually experiences: the weakness or paralysis of the arm that results from that damage.
Recognizing the Symptoms
Brachial plexus injury symptoms don’t always announce themselves dramatically. A football player might feel a brief electric jolt down the arm that clears within minutes. A trauma patient might wake up unable to lift their arm at all. The severity of presentation reflects the severity of the underlying injury, but the distribution of symptoms carries diagnostic information beyond severity alone.
Common presentations include numbness or tingling from the shoulder to the fingertips, weakness in shoulder elevation or elbow flexion, inability to raise the arm overhead, wrist drop, reduced grip strength, and complete paralysis of the limb. Burning or electric shock-like pain radiating from the neck into the hand is also characteristic, particularly in stretch and avulsion injuries.
The pattern of deficits helps localize the injury: upper plexus involvement (C5–C6) primarily affects shoulder movement and elbow flexion; lower root damage (C8–T1) presents as weakness in the hand and grip.
How Neurologists Diagnose Brachial Plexus Injuries

Diagnosis begins with a systematic neurological exam. The physician tests muscle strength across every major upper extremity movement and maps sensory changes through the dermatomal territories of C5 to T1. This examination alone can localize an injury with considerable accuracy before any imaging is ordered.
Electrodiagnostic testing, EMG combined with nerve conduction studies, provides objective data that the clinical exam cannot. These studies are performed three to four weeks after injury, not immediately. The reason matters: the denervation changes that make EMG results clinically meaningful take time to develop. Testing too early produces incomplete and potentially misleading findings.
For structural evaluation, MRI neurography visualizes nerve continuity, swelling, and scarring. When avulsion is suspected, CT myelography provides the clearest picture of root integrity before any surgical planning begins.
No single test tells the whole story. A thorough workup for brachial plexus injury integrates the neurological exam, electrodiagnostic testing, and imaging – each contributing a layer that the others cannot replace.
Treatment and Recovery Options
The diagnostic workup determines treatment, and timing matters more than most patients realize.
For mild stretch injuries (neuropraxia), the approach is conservative: observation, physical therapy to maintain joint mobility, and time. The nerve can heal itself; the clinical goal is to preserve muscles and joints while it does.
For more severe injuries, brachial plexus injury treatment should ideally begin within three to six months of trauma. Beyond that window, denervated muscles progressively lose their capacity to respond even after successful nerve repair. Surgical options include nerve grafting, bridging a gap with a donor nerve segment, nerve transfer (redirecting a healthy nearby nerve to take over the injured root’s function), and, in later-stage cases, tendon or muscle transfers to restore specific movements when nerve repair is no longer viable.
Brachial plexus injury recovery is slow by biological necessity. Nerves regenerate at approximately one inch per month. After nerve transfer surgery, early motor signs typically emerge at 6 to 12 months, with full recovery, when achievable, taking 2 to 4 years. Rehabilitation that begins early consistently produces better outcomes than delayed intervention.
When to See a Neurologist After a Shoulder or Arm Injury
Seek neurological evaluation after trauma if you notice: weakness or numbness in the arm or hand, inability to lift the shoulder or close the fingers, burning pain shooting from the neck down into the limb, or no functional improvement after several weeks.
The window for surgical intervention is real and finite. Early nerve testing – EMG performed at the right time – is what guides the decision between observation and surgery while both options remain on the table.
At Lone Star Neurology, our team performs comprehensive EMG and nerve conduction studies across 18 DFW locations. If an injury is affecting arm or hand function, we can evaluate brachial plexus nerve damage with the diagnostic precision needed to determine the right path forward.
FAQ
Can a brachial plexus injury heal on its own?
Mild stretch injuries (neuropraxia) often do. The nerve’s insulating sheath is temporarily disrupted but structurally intact, and most patients regain full function within days to weeks without intervention. Injuries involving torn axons, complete nerve tears, or avulsion from the spinal cord will not heal without surgical treatment.
How long does it take to recover from a brachial plexus injury?
It depends entirely on severity. A stinger in a contact sport may clear in minutes. Partial tears typically require six months to two years of recovery. After nerve transfer surgery, early signs of motor recovery usually appear at 6 to 12 months, but full functional recovery, when achievable, can take 2 to 4 years.
Is brachial plexus injury permanent?
It can be. Avulsion injuries – where the nerve root is separated from the spinal cord – produce permanent deficits without nerve transfer surgery, and even after surgery, recovery is typically partial. Mild injuries carry an excellent prognosis with appropriate and timely care.
What is the difference between brachial plexopathy and brachial plexus palsy?
Brachial plexopathy refers to the underlying dysfunction of the brachial plexus network – the pathological process itself. Brachial plexus palsy describes the resulting clinical deficit: the weakness or paralysis the patient experiences. One names the diagnosis; the other describes the consequence.
When is surgery needed for a brachial plexus injury?
Surgery is indicated when nerve fibers are completely torn (neurotmesis), when avulsion is confirmed on imaging, or when there is no meaningful functional recovery after an appropriate observation period. The decision is typically made between three and six months post-injury, based on a combination of EMG findings, clinical exam, and imaging results.
 (No Ratings Yet)
(No Ratings Yet)







I've given up... the stress her office staff has put me through is just not worth it. You can do so much better, please clean house, either change out your office staff, or find a way for them to be more efficient please. You have to do something. This is not how you want to run your practice. It leaves a very bad impression on your business.
Please, leave your review
Write a comment: