

Cervical (carotid) artery dissection (CAD) is a rupture of a layer of the artery wall, in which blood begins to seep and spread between the layers. It is responsible for 20% of ischemic strokes in adults diagnosis under 45 years old, accounting for 2% of all IS.
CAD is rare – the frequency of dissection of the cervical artery is 2.5-3 cases per 100 thousand population per year, vertebral artery dissection (VAD) – 1-1.5 cases per 100 thousand population per year. In the course of aging, many other factors contribute to the development of IS. Therefore, it is believed that CAD is the cause of only 2-3% of all IS in elderly patients; however, in this population, spontaneous CAD is usually rarely diagnosed unreasonably.
In fact, in stroke, arterial dissection was the most relevant cause of headache; a recent study found that up to 8% of patients with spontaneous ASD experience headache or neck pain as the first symptoms of a stroke.
There are no significant sex differences, but the condition develops on average about 5 years earlier in women than in men. Most often, dissection occurs in the most mobile areas of the carotid and vertebral arteries, which emphasizes the importance of accompanying mechanical factors in the pathogenesis of spontaneous CAD.
- Recurrent spontaneous CAD is a rare phenomenon and, according to previous studies, is observed in 3–8% of cases.
- It is noteworthy that, according to new evidence, delayed relapses are more frequent than previously thought and may develop at the level of the previous stratification.
- Among patients with spontaneous cervical artery dissection, the risk of re-dissection was reported to be 3% during a mean follow-up of 36 months and reached 8% in a study with a mean follow-up of 7.4 years with the highest relapse rate (2%) during the first months after the primary event.
However, relapse rates are difficult to estimate, as relapse is sometimes asymptomatic, especially if it occurs within a few weeks, and dissections with isolated local symptoms are likely to be unreasonably rare to be diagnosed.
According to a large multicenter study, the incidence of symptomatic recurrence of CAD is 0.3% per year, which is slightly less than reported in earlier studies, in which relapses were most common among patients with connective tissue diseases or family history of CAD.

Cervical artery dissection causes and diagnostics
Causes
The main provoking factors for dissection are:
- head or neck trauma (primarily as a result of accidents), usually mild;
- physical activity with muscle tension in the shoulder girdle and neck;
- tilts and turns of the head;
- alcohol intake;
- current or previous infection;
- taking contraceptives;
- the postpartum period in women.
Diagnosis
Diagnosis of cervical artery dissection is mainly based on the results of angiographic methods:
- magnetic resonance imaging (MRI);
- spiral computed angiography (SCT-AG);
- radiopaque angiography (RA);
- ultrasound by color duplex scanning (CDS).
Dissection by intramural hematoma with hemodynamically significant stenosis of the ICA at the extracranial level, thrombosis of the ICA distal to the dissection area, and “candle flame symptom” – CDS, Doppler curve, and DSA.
- MRI of the neck vessels in the area of the internal carotid artery dissection shows a high signal from the vessel wall, no signal, and bending of the vessel. With MRI of the brain, the consequences of dissection of the carotid arteries, territorial extensive strokes, are clearly visible.
- SCT-AG combines two methods: slip ring CT scanning and computerized three-dimensional (3D) reconstruction.
- Radiopaque angiography is a method for diagnosing vascular diseases, in which a contrast agent is injected into them, staining its lumen. The passage of contrast through the vessels is monitored on a special apparatus – an angiograph.
- Thanks to CDS, you can obtain information about the quality of blood flow, as well as the presence of anatomical or postoperative abnormalities, the appearance of blood clots, the geometry of the vascular lumen, wall thickness, channel tortuosity, and atherosclerotic plaques.

Carotid (cervical) artery dissection treatment
Treatment of a cervical artery is not definitively defined, as there are no randomized, placebo-controlled trials involving large numbers of patients. In this regard, there are no clearly established methods of treatment of a cervical artery in the acute period of stroke.
- Most often, it is recommended to introduce direct anticoagulants, followed by a switch to indirect anticoagulants, used for 3–6 months:
- their purpose is to prevent arterio-arterial embolism;
- people should bear in mind that the appointment of large doses of anticoagulants can lead to a deterioration in the blood supply to the brain.
- As an alternative to these drugs in the acute period of stroke, the use of antiplatelet agents is recommended, while there are no differences in stroke outcomes, according to preliminary data:
- to assess the safety of treatment with low molecular weight heparin and aspirin in the acute period of dissection, French researchers measured the volume and extent of IMH during the 1st week of treatment of a cervical artery;
- a slight increase in these parameters was observed in one-third of patients, but in none of the cases was there an increase in the degree of stenosis or the development of repeated dissection;
- the use of anticoagulants and antiplatelet agents is limited to 2-3 months;
- further prophylactic use of these drugs is inappropriate since the cause of dissection of the cervical artery is not hypercoagulation but the weakness of the arterial wall.
Since the main reason predisposing to the development of dissection is the weakness of the arterial wall, therapeutic measures both in the acute and in the long-term period of stroke should be aimed at strengthening it. If we take into account the data on mitochondrial cytopathy, which leads to energy deficiency of cells of the arterial wall and its dysplasia, which contributes to the onset of dissection, the use of drugs with energotropic action can be considered justified.
- One of these drugs is Actovegin, which is used both in the acute and in the long-term period of stroke caused by dissection. It is a biologically active substance of natural origin – a deproteinized derivative of calf blood. The main action of Actovegin is to activate cellular metabolism by facilitating the flow of oxygen and glucose into the cell, which provides an additional influx of energy substrates and increases by 18 times a universal donor of energy necessary for the vital activity and functioning of the cell.
- Other drugs with a neurometabolic effect are also used to restore functions impaired due to a stroke: cerebrolysin, piracetam, gliatilin, ceraxon.
In the acute period of dissection, in addition to drug treatment, it is of great importance to observe the following rules:
- avoid sudden head movements;
- avoid injuries;
- avoid physical stress;
- avoid straining, which can lead to an increase in dissection.
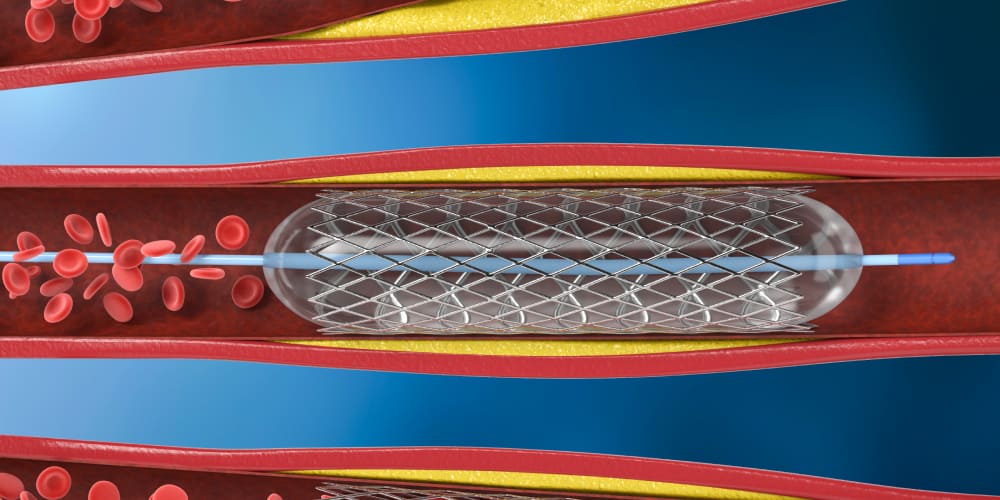
Carotid artery dissection endovascular therapy presenting with ischemic stroke
Endovascular treatment is widely used to treat cardiovascular and cerebrovascular diseases.
- Endovascular therapy can effectively improve vascular stenosis caused by coronary artery disease and reduce the incidence of ischemic stroke;
- Also, multiple overlapping stents can effectively reduce blood flow velocity in pseudoaneurysms and promote thrombosis, thereby reducing or causing pseudoaneurysms to disappear.
Endovascular therapy:
- Is mainly used in patients with coronary artery disease with ineffective antithrombotic treatment with contraindications for anticoagulation and pseudoaneurysm, as well as when stent implantation is the main procedure for vascular intervention.
- Endovascular/surgical treatment of cervical artery disease should be limited because patients with coronary artery disease have a lower risk of recurrent ischemic stroke.
- There is no significant correlation between coronary artery disease-induced vascular stenosis and pseudoaneurysm, and endovascular/surgical treatments are traumatic. Endovascular treatment can be considered the preferred treatment option for patients with coronary artery disease, especially when the patient has both embolism and obvious hypoperfusion. In this case, endovascular therapy can effectively reduce stenosis, increase blood flow, and improve low perfusion.
- In a retrospective study, 140 patients with coronary artery disease underwent stenting, and angiographic observation was carried out for an average of 12.8 months. The results showed that vascular stenosis caused by dissection was significantly reduced and that secondary strokes accounted for only 1.4% of cases.
- Previous studies have shown that dissection stenosis in patients with coronary artery disease undergoing stent therapy can be significantly reduced – from 71% to complete remission.
Carotid artery dissection prognosis
The prognosis for life in most cases is favorable. Fatality, according to our information and data literature, is observed in about 5% of cases. Usually, it occurs with extensive cerebral infarctions caused by dissection of the intracranial part of the Internal Carotid Artery (ICA) with the transition to the Middle cerebral artery (MCA) and the cervical artery.
- In most patients the prognosis for life is favorable and there is a good recovery of the impaired functions.
- When there is the involvement of the intracranial part of the ICA and dissection spread to the MCA or with embolism of the last restoration of impaired functions, the prognosis is much worse:
- dissection recurs infrequently and is usually present in the 1st month after the onset of the disease. They can appear both intact and already dissected arteries;
- the main mechanism of IS development is hemodynamic under conditions of an increasing stenosing-occlusive process in the ICA due to myocardial infarction;
- less commonly, an intrauterine device (IUD) develops by the mechanism of arterial embolism;
- its source is blood clots that form in a dissecting aneurysm, thrombosed imaging fragments that enter the bloodstream with a secondary breakthrough of the intima, or thrombotic layers at the site of rupture of the intima.
The available data stimulates researchers to better understand the pathological physiology of CAD and to focus on environmental and genetic risk factors. Modern methods of treatment and prevention are likely to be effective in modifying the natural course of this disease.
FAQ
- Is a car accident an important risk factor for cervical (carotid) artery dissections?
Yes, it is a dangerous factor for cervical (carotid) artery dissections. The injured people of car accidents should be examined.
- What is carotid dissection?
Dissection is the penetration of blood through the intimal gap from the lumen of the artery into its wall with the formation of an intramural hematoma (IMH), which stenoses / occludes the lumen of the artery or is a source of arterio-arterial embolism, which in turn leads to ischemic stroke.
- What is the main reason of cervical (carotid) artery dissection?
Since the main reason predisposing to the development of dissection is the weakness of the arterial wall, therapeutic measures both in the acute and in the long-term period of stroke should be aimed at strengthening it.
- Can you die from cervical artery syndrome?
Cervical artery syndrome is a life-threatening emergency requiring urgent medical attention. Even if the illness lasts for decades, you should not wait and test your luck. 80% of patients can be cured of pathology, the remaining 20% get better.
- What is cervical artery stenosis?
Stenosis of the cervical spine is a process of reducing the lumen of the spinal canal due to the development of various pathological structures. As a rule, the tendency to form stenosis is most often manifested in people over 55 years of age.
 (No Ratings Yet)
(No Ratings Yet)





I've given up... the stress her office staff has put me through is just not worth it. You can do so much better, please clean house, either change out your office staff, or find a way for them to be more efficient please. You have to do something. This is not how you want to run your practice. It leaves a very bad impression on your business.
Please, leave your review
Write a comment: